

Good news for all those families Fighting Cancer that Cipla Slashed Prices of Life Saving Cancer Medicines. I am not sure whether the Medical practitioners would be in a mood to care enough for Pricing Cheaper medicines at the cost of the Commission and incentives they get for Multi National Companies.We have faced Two Deaths from Cancer in our family already. My Aunt died in 1995 in Sodepur before our helpless eyes and we could not save my Father, the life long Struggler Pulin Babu from Spinal Chord Cancer!It is a special newsbreak for us all, no doubt. But I am afraid that it may turn to be a super super Marketing Strategy like the Corporate Philanthropy!
Indian Holocaust My Father`s Life and Time - Eight HUNDRED THIRTY Two
Palash Biswas
http://indianholocaustmyfatherslifeandtime.blogspot.com/
http://basantipurtimes.blogspot.com/
Good news for all those families Fighting Cancer that Cipla Slashed Prices of Life Saving Cancer Medicines. ! am not sure whether the Medical practitioners would be in a mood to care enough for Pricing Cheaper medicines at the cost of the Commission and incentives they get for Multi National Companies.We have faced Two Deaths from Cancer in our family already. My Aunt died in 1995 in Sodepur before our helpless eyes and we could not save my Father, the life long Struggler Pulin Babu from Spinal Chord Cancer!It is a special newsbreak for us all, no doubt. But I am afraid that it may turn to be a super super Marketing Strategy like the Corporate Philanthropy!
My aunt Mrs Usha Devi was admitted in Bishuddhanand Marwari Hospital with a complain against acute Pain in stomoch. The doctors diaognised stones in the spleen and she was operated. The Biopsy report exposed the spreading Cancer. We carried her to the Thakur Pukur Cancer Hospital and they could not help much. We had to wait for her death. it was unbearable situation as she was suffering so much so acute pain. My Cousine and his wife were so much strained that they could not stand beside her. Sabita had to stay with them. I Channelised myself in creative writing as I was writing my Novel AMERICA Se Savdhan which was being Published in serial in Dainik Awaz in Dhanbad and Jamshedpur and parts of which were being published in scores of little mags countrywide.My aunt had to survive on Morphyn!Within weeks she succumbed.
I was away in Manipur, shooting for Joshy Joseph`s film IMAGINARY Lines while doctors in Sushila devi hospital diognised cancer. I had to rush home and carry my Father to All India Medical Institute , New Delhi.Thanks to media support and initiative by KC pant, a medical board was constituted and they could not help. My father had to survive with Homeo Medicines which reduced his pain a little bit.
We understand the suffering and pain very well. My friend dilip Mandal`s wife Anuradha Defeated Cancer and later she rote a book on her experience. The latest case is about Cricket Icon, Yuvraj Singh. It is an excellent story of fighting against Cancer. But the fact remains that the support yuvraj gets as an Icon, the Common Man , may not dream of. Rather the Common Man has to fight against the Medical and drug Mafias at a time before beginning his fight against the ailment.
Cipla's generic Sorafenib, which is used by patients suffering from kidney cancer, will now be available for Rs 6,840 as opposed to its earlier price Rs 27,950.
Furthermore, the company has slashed prices for its lung cancer drug Gestinib by 60%. The drug will now be sold for Rs 4,250 compared to its earlier cost of Rs 10,200.
Additionally, Cipla has also reduced the price for Temozolamide, a drug used to cure brain tumour. Post price reductions, 20mg, 100mg and 250mg of Temozolamide will be available for Rs 1,875, Rs 2,400 and Rs 5,000 respectively.
There is more than this happening for the company, as the renowned financial group CLSA upgraded its rating to 'outperform' and set a target of Rs 360 per share.
According to CLSA, one can expect stronger operating performance by Cipla over the coming quarters, along with margin expansion on the back of high margin product supplies. The firm further pointed that partner Meda's approval for the drug Dymista, which can treat seasonal allergic rhinitis, will add to the company's earnings. CLSA says Cipla could earn around $50- 75 million at peak sale from Dymista.
Moreover, with the rupee depreciating every day, Cipla has benefitted significantly. The company has also been showing signs of an improving domestic market according to the All India Organisation of Chemists and Druggists (AIOCD) data. CLSA pointed out that after the company's recent corrections in the Indian market, the valuations look attractive.
Drug major Cipla has slashed by up to 76% the prices of certain life-saving cancer drugs used in the treatment of brain, lung and kidney cancer. On the other hand, Shares in Cipla (CIPL.NS) gain 3.1 percent to 327.35 rupees after CLSA upgrades the stock to "outperform" from "underperform", maintaining its 12-month price target at 360 rupees.The brokerage says it expects "strong" operating performance from Lexapro, an anxiety and depression drug, and a weaker rupee.t's a drug war, but with a difference and it's been kicked off by Cipla . CNBC TV18's Archana Shukla reports that country's second largest drug firm has slashed prices of three of its key cancer drugs by more than half, making cancer medication costs come down by over 50%.
CLSA says nasal spray Dymista will also boost earnings as U.S. sales ramp up. The brokerage also calls Cipla's valuations "reasonable" after recent sharp falls.
Separately, Cipla has cut the price of some of its cancer drugs, but company says no impact seen on revenues due to very low volumes of these drugs.
The move comes on the back of the government allowing domestic firm Natco Pharma to sell generic version of cancer drug Nexavar at nearly 97% lower price than charged by patent-holder Bayer Corporation. In March, the Indian Patent Controller cleared Natco's application to sell the drug at Rs 8,880 for a month's treatment, as compared to Rs 2.8 lakh per month charged by Bayer for its patented Nexavar drug.
The price of Cipla's 'Soranib', used for treating kidney cancer, has been reduced by 76% to Rs 1,710 for a month's therapy, from Rs 6,990, the company said in a statement.
Brain cancer drug 'Temoside' in 250 mg strength would be available at Rs 5,000 against Rs 20,250 earlier, a reduction of 75%. Lung cancer drug Gefticip 250 mg in packs of 10 and 30 tablets will be priced 59% cheaper at Rs 1,555 and Rs 4,250, as against their existing prices of Rs 3,400 and Rs 10,200, respectively, it added.
Cipla chairman and managing director YK Hamied said, "This initiative of price reduction is a humanitarian approach by Cipla to support cancer patients." Drugs constitutes a significant proportion of the overall cost of cancer treatment and reduction in costs can greatly relieve the burden, he added.
Cipla has a known affinity for cheaper drugs, and after tasting success with cheaper generics in the anti-HIV space, it has turned its attention to the battle against cancer.
Cipla has slashed prices of kidney cancer drug, generic Sorafenib by 75% to Rs 6,840 per month. Prices of Geftinib, generic version of Astrazeneca's lung cancer drug, have been cut by 60% and for generic version of Schering's brain tumour drug Temozolamide by 75%.
Strategically, Cipla's move comes at a time when the Indian Govt is trying to make cancer drugs cheaper, and will stir up competition in the Rs 1,500 crore segment.
In a recent historic ruling, Indian drug firm Natco was granted a compulsory licence by the Indian Patent Office to market generic Sorafenib (Nexavar) At Rs 8,900 per month, against patent holder Bayer's price of Rs 2.8 lakh.
And while Cipla is yet to resolve the patent infringement case filed by Bayer on generic Sorafenib, its move to slash prices of its drugs will see it taking on Natco head on.
So, what does Natco make of this move?
Bhaskar Narayana, Director - Finance & CFO, Natco Pharma told CNBC TV 18, "Natco got a compulsory licence which gives us authority to manufacture and market this product. As far as we know Cipla does not have this kind of an authority. Notwithstanding this we welcome this competition because it is what was required in the Indian context."
The Indian Patent Office's stance on compulsory licences has made multinationals review their pricing strategies to safeguard their patent rights in India. Recently, Swiss drug giant Roche said it would lower prices of two of its blockbuster anti-cancer drugs Mabthera and Herceptin, based on a tie-up with Indian firm Emcure for local packaging of these drugs, so as to cut costs.
Some speculate that Cipla's price cuts could also be a precursor to its plans of filing for compulsory licences for some of these products. But as analysts point out, the first benefit will certainly be for cancer patients who will now have to pay significantly less for their medication and
treatment.
Considering the growing number of cancer cases in the state, the Kerala state government has initiated a cancer care project to set up early detection and management centres for cancer in all districts where such facilities are not available. The project also envisages early cancer detection camps in vulnerable areas, provision for free medicines and setting up of infrastructure for the detection of breast and oral cancers.
In the first phase of the project, a sum of `5 crore has been allotted in the 2012-13 budget. Cancer detection and management centres will be opened at the general hospitals in six districts. In these centres there will be facilities for chemotherapy and medical care. A doctor, a nurse and a lab technician from each of these hospitals will be given six months' training at the Regional Cancer Centre (RCC), Thiruvananthapuram.
"The aim of the project is to reduce the burden of travel on the patients who have to depend on prominent cancer care hospitals for the treatment," said Dr Vipin Gopal, state nodal officer for the programme. A mammography detection unit will be set up at Thiruvananthapuram Medical College to diagnose breast cancer. As of now, the facility is available only at Ernakulam General Hospital in the public sector. Moreover, oral cancer detection centres will be opened in five districts of the state.
Apart from this, there are plans to conduct two cancer detection camps in the tribal regions of all districts. This is on account of the high prevalence and low detection of oral cancer among tribal population in the state. The prevalence of non-smoking tobacco use is the main reason for the high incidence of oral cancer among the tribal people.
According to the figures available with the Health Department, as many as 1 lakh patients are being treated for cancer in the state and 35,000 patients are added to this every year.
Meanwhile, a prebiotic has shown promise in helping the body`s own natural killer cells fight bacterial infection and lower colon cancer risk, a study says.Prebiotics are dietary fibre supplements that serve as food for the trillions of tiny bugs living in the gut and stimulate the growth of the "good" bacteria.
The evolution of prebiotic supplements (as well as probiotics, actual bacteria ingested into the system) provide new therapeutic targets for researchers and physicians, the Journal of Nutrition reports.
Jenifer Fenton, a researcher at Michigan State University, US, reports that mice given the prebiotic galacto-oligosaccharide, or GOS, saw the severity of their colitis (an inflammatory bowel disease) significantly reduced. Inflammation is the immune system`s response to illness, infection, according to a Michigan statement.
Colon cancer symptoms can run the gamut from local, such as blood in the stool and constipation, to systemic, such as weight loss and fatigue.
In fact, the mice fed GOS - a synthetic compound that is known to stimulate beneficial bacteria and is found in foods such as biscuits and infant formula - saw a 50 percent reduction in colitis.
Research has shown certain types of foods and fibres can reduce colon cancer risk, said Fenton, researcher in food science.
"There is something unique about certain types of fibres, such as GOS, and how they alter cells and influence the immune system to change disease risk, either for the good or bad," Fenton said.
"Our overall goal is to identify either dietary patterns or diet components to reduce inflammation and cancer risk. In this case, we used prebiotics to stimulate changes in bacteria in the gut that may have a beneficial impact on the colon," the Michigan researcher added.
"Our results suggest GOS may be effective in reducing colitis severity by priming the innate immune system," she said.
The next step is to verify how that mechanism works; finding that link could help researchers apply the lessons learned to other intestinal ailments.
More than 40,000 men are being diagnosed with prostate cancer in the UK every year, figures show.
The number of new cases annually has almost trebled since 1989 when it stood at 14,000, according to the charity Cancer Research UK.
This increase is mainly due to greater use of the Prostate Specific Antigen (PSA) test, which measures levels of a chemical that is high when tumours are present.
But although the test has been credited with detecting some deadly cancer cases earlier, there are concerns it often causes 'false alarms'.
Some two-thirds of men with raised PSA levels do not have prostate cancer. They are forced to undergo further unpleasant examinations to determine whether or not they have the illness.
'I've dreamed in colour for the first time in 20 years': Blind British man can see again after first successful implant of 'bionic' eye microchips
Coldest of cold cases: Scientists recover world's oldest blood sample from a murder victim preserved in ice for 5,000 years
And even these checks will not necessarily determine whether or not the cancer is aggressive and life-threatening.
It means that thousands of men will undergo surgery, chemotherapy or radiotherapy – which have debilitating side-effects – for cancers which may never have caused a problem.
Warning: Professor Malcolm Mason, Cancer Research UK's prostate cancer expert
Professor Malcolm Mason, of Cancer Research UK, said: 'Accurately diagnosing and predicting the need for treatment of prostate cancer is fraught with difficulties and there is no escaping the fact that we need a better tool than PSA to help detect prostate cancers that actually need treating.
'Men need to be counselled about the upsides and downsides of having a PSA test and the uncertainties that it can raise.
'We urgently need to find better tests that tell us more about a man's prostate cancer. Is the disease going to sit quietly in the background and never cause a problem or do we need to treat it aggressively?
'If we can accurately answer these questions, we could spare thousands of men unnecessary treatment that can lead to side-effects like impotence and incontinence.'
Earlier this week American researchers claimed that surgery to remove prostate cancer is often ineffective. A study involving 731 patients found that those who had operations were only 3 per cent more likely still to be alive 12 years later compared to those who didn't have treatment.
The researchers from the University of Minnesota said this increase could well be down to chance.
Complex: Prostate cancer cells can be slow growing with no radical treatment needed, but in others, early surgery or radiotherapy is vital
There is no national screening programme for prostate cancer in the UK but men who want a PSA test can request one from their GP.
Figures from Cancer Research UK also show that the death rate from prostate cancer has fallen by 11 per cent in the past ten years.
Prostate cancer is the second most common form of the illness in men after lung cancer. Although it leads to 10,000 deaths a year, in about 50 per cent of cases the cancer is growing so slowly it is not life-threatening.
The PSA test involves a sample of blood being taken and measured for levels of the prostate specific antigen.
But there are many reasons why readings can be high and it is not necessarily due to the presence of cancer.
A urine infection can lead to a positive result, for example. And some men have subsequently been diagnosed with cancer even though their PSA test was normal.
Earlier this year the NHS rationing body NICE controversially decided to reject a drug for advanced prostate cancer even though it can give patients precious extra months of life.
The watchdog ruled in February that abiraterone was too expensive for use in England at £35,000 per patient per year.
Read more: http://www.dailymail.co.uk/health/article-2139078/Prostate-cases-treble-20-years-But-diagnosed-cancer-fewer-men-die.html#ixzz1tt9zllhX
Ann Romney opened up about her battle with breast cancer, saying the disease made her "see others in a different light." She spoke in a surprisingly candid interview Thursday with America's Radio Network.
Romney was diagnosed with cancer in January 2009. Her husband, presumptive Republican presidential nominee Mitt Romney, "was with me when I got my diagnosis of MS, and then he was with me again when I got the call that my results were back, and that I did have cancer," Ann Romney said. "You just fight these battles. ... Listen, you don't fight them alone, you fight them with friends and family."
Tragically for Romney, cancer had already played a big role in her life.
"I lost my mother from ovarian cancer, I lost my grandmother from ovarian cancer, I lost my great grandmother from breast cancer," she said. "It's been a long line of cancer, women that have death with cancer in their lives."
Romney praised U.S. breast cancer research and emphasized the importance of early diagnosis.
When asked whether she worries about cancer returning, she admitted to holding her breath for every screening. Still, she said she celebrated each day.
"Life is an interesting game," she said. "Sometimes you just deal with the cards that are dealt you. And you just go on. You just push forward."
She said she was overwhelmed by the immense love and support she felt while struggling with the illness. "You'll find out how wonderful people are, and how generous people are, and how caring people are, and how we all belong to this race of humanity," she said. "For me, it's opened my heart up and made me see others in a different light."
Romney called the diagnosis a "blessing" for what it taught her. She said coping with difficult situations is an unavoidable part of life.
"We all will be dealt a challenge," she said. "We can't escape life without facing these."
http://www.huffingtonpost.com/2012/05/03/ann-romney-breast-cancer_n_1475950.html
Cancer
Carcinoma; Malignant tumorLast reviewed: August 14, 2010.
Cancer is the uncontrolled growth of abnormal cells in the body. Cancerous cells are also called malignant cells.
Causes, incidence, and risk factors
Cells are the building blocks of living things.Cancer grows out of normal cells in the body. Normal cells multiply when the body needs them, and die when the body doesn't need them. Cancer appears to occur when the growth of cells in the body is out of control and cells divide too quickly. It can also occur when cells forget how to die.
There are many different kinds of cancers. Cancer can develop in almost any organ or tissue, such as the lung, colon, breast, skin, bones, or nerve tissue.
There are many causes of cancers, including:
- Benzene and other chemicals
- Drinking excess alcohol
- Environmental toxins, such as certain poisonous mushrooms and a type of poison that can grow on peanut plants (aflatoxins)
- Excessive sunlight exposure
- Genetic problems
- Obesity
- Radiation
- Viruses
The most common cause of cancer-related death is lung cancer.
The three most common cancers in men in the United States are:
- Colon cancer
- Lung cancer
Some other types of cancers include:
- Skin cancer
Symptoms
Symptoms of cancer depend on the type and location of the cancer. For example, lung cancer can causecoughing, shortness of breath, or chest pain. Colon cancer often causes diarrhea, constipation, and blood in the stool.Some cancers may not have any symptoms at all. In certain cancers, such as pancreatic cancer, symptoms often do not start until the disease has reached an advanced stage.
The following symptoms can occur with most cancers:
- Night sweats
Signs and tests
Like symptoms, the signs of cancer vary based on the type and location of the tumor. Common tests include the following:- Biopsy of the tumor
- Blood tests (which look for chemicals such as tumor markers)
- Bone marrow biopsy (for lymphoma or leukemia)
- Complete blood count (CBC)
A cancer diagnosis is difficult to cope with. It is important, however, that you discuss the type, size, and location of the cancer with your doctor when you are diagnosed. You also will want to ask about treatment options, along with their benefits and risks.
It's a good idea to have someone with you at the doctor's office to help you get through the diagnosis. If you have trouble asking questions after hearing about your diagnosis, the person you bring with you can ask them for you.
Treatment
Treatment varies based on the type of cancer and its stage. The stage of a cancer refers to how much it has grown and whether the tumor has spread from its original location.- If the cancer is confined to one location and has not spread, the most common treatment approach is surgery to cure the cancer. This is often the case with skin cancers, as well as cancers of the lung, breast, and colon.
- If the tumor has spread to local lymph nodes only, sometimes these can be removed.
- If surgery cannot remove all of the cancer, the options for treatment include radiation, chemotherapy, or both. Some cancers require a combination of surgery, radiation, and chemotherapy.
- Lymphoma, or cancer of the lymph glands, is rarely treated with surgery. Chemotherapy and radiation therapy are most often used to treat lymphoma.
If you have radiation treatment, know that:
- Radiation treatment is painless.
- Treatment is usually scheduled every weekday.
- You should allow 30 minutes for each treatment session, although the treatment itself usually takes only a few minutes.
- You should get plenty of rest and eat a well-balanced diet during the course of your radiation therapy.
- Skin in the treated area may become sensitive and easily irritated.
- Side effects of radiation treatment are usually temporary. They vary depending on the area of the body that is being treated.
It will help you to talk with family, friends, or a support group about your feelings. Work with your health care providers throughout your treatment. Helping yourself can make you feel more in control.
Support Groups
The diagnosis and treatment of cancer often causes a lot of anxiety and can affect a person's entire life. There are many resources for cancer patients.See: Cancer resources
Expectations (prognosis)
The outlook depends on the type of cancer. Even among people with one type of cancer, the outcome varies depending on the stage of the tumor when they are diagnosed.Some cancers can be cured. Other cancers that are not curable can still be treated well. Some patients can live for many years with their cancer. Other tumors are quickly life-threatening.
Complications
One complication is that the cancer may spread. Other complications vary with the type and stage of the tumor.Calling your health care provider
Contact your health care provider if you develop symptoms of cancer.Prevention
You can reduce the risk of getting a cancerous (malignant) tumor by:- Eating a healthy diet
- Exercising regularly
- Limiting alcohol
- Maintaining a healthy weight
- Minimizing your exposure to radiation and toxic chemicals
- Not smoking or chewing tobacco
- Reducing sun exposure, especially if you burn easily
References
- Moscow JA, Cowan KH. Biology of cancer. In: Goldman L, Ausiello D, eds. Cecil Medicine. 23rd ed. Philadelphia, Pa: Saunders Elsevier;2007:chap 187.
- Thun MJ. Epidemiology of cancer. In: Goldman L, Ausiello D, eds. Cecil Medicine. 23rd ed. Philadelphia, Pa: Saunders Elsevier;2007:chap 185.
Review Date: 8/14/2010.
Reviewed by: David C. Dugdale, III, MD, Professor of Medicine, Division of General Medicine, Department of Medicine, University of Washington School of Medicine. Also reviewed by David Zieve, MD, MHA, Medical Director, A.D.A.M., Inc.
http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0002267/
Cancer
From Wikipedia, the free encyclopediaFor other uses, see Cancer (disambiguation).

| Cancer | |
| Classification and external resources | |
 * * | |
Cancer /ˈkænsər/ (listen), known medically as a malignant neoplasm, is a broad group of various diseases, all involving unregulated cell growth. In cancer, cells divide and grow uncontrollably, forming malignant tumors, and invade nearby parts of the body. The cancer may also spread to more distant parts of the body through the lymphatic system or bloodstream. Not all tumors are cancerous. Benign tumors do not grow uncontrollably, do not invade neighboring tissues, and do not spread throughout the body.
Determining what causes cancer is complex. Many things are known to increase the risk of cancer, including tobacco use, certain infections, radiation, lack of physical activity, poor diet and obesity, and environmental pollutants.[1] These can directly damage genes or combine with existing genetic faults within cells to cause the disease.[2] Approximately five to ten percent of cancers are entirely hereditary.
Cancer can be detected in a number of ways, including the presence of certain signs and symptoms, screening tests, or medical imaging. Once a possible cancer is detected it is diagnosed by microscopic examination of a tissue sample. Cancer is usually treated withchemotherapy, radiation therapy and surgery. The chances of surviving the disease vary greatly by the type and location of the cancer and the extent of disease at the start of treatment. While cancer can affect people of all ages, and a few types of cancer are more common in children, the risk of developing cancer generally increases with age. In 2007, cancer caused about 13% ofall human deaths worldwide (7.9 million). Rates are rising as more people live to an old age and as mass lifestyle changes occur in the developing world.[3]
Signs and symptoms
Main article: Cancer signs and symptomsWhen cancer begins it invariably produces no symptoms with signs and symptoms only appearing as the mass continues to grow or ulcerates. The findings that result depends on the type and location of the cancer. Few symptoms are specific, with many of them also frequently occurring in individuals who have other conditions. Cancer is the new "great imitator". Thus it is not uncommon for people diagnosed with cancer to have been treated for other diseases to which it was assumed their symptoms were due.[4]
Local effects
Local symptoms may occur due to the mass of the tumor or its ulceration. For example mass effects from lung cancer can cause blockage of the bronchus resulting in cough or pneumonia,esophageal cancer can cause narrowing of the esophagus making it difficult or painful to swallow, and colorectal cancer may lead to narrowing or blockages in the bowel resulting in changes in bowel habits. Masses of breast or testicles may be easily felt. Ulceration can cause bleeding which, if it occurs in the lung, will lead to coughing up blood, in the bowels to anemia or rectal bleeding, in the bladder to blood in the urine, and in the uterus to vaginal bleeding. Although localized pain may occurs in advanced cancer, the initial swelling is usually painless. Some cancers can cause build up of fluid within the chest or abdomen.[4]Systemic symptoms
General symptoms occur due to distant effects of the cancer that are not related to direct or metastatic spread. These may include: unintentional weight loss, fever, being excessively tired, and changes to the skin.[5] Hodgkin disease,leukemias, and cancers of the liver or kidney can cause a persistent fever of unknown origin.[4]Specific constellations of systemic symptoms, termed paraneoplastic phenomena, may occur with some cancers. Examples include the appearance of myasthenia gravis in thymoma and clubbing in lung cancer.[4]
Metastasis
Symptoms of metastasis are due to the spread of cancer to other locations in the body. They can include enlarged lymph nodes (which can be felt or sometimes seen under the skin and are typically hard), hepatomegaly (enlarged liver) or splenomegaly (enlarged spleen) which can be felt in the abdomen, pain or fracture of affected bones, and neurological symptoms.[4]Causes
Cancers are primarily an environmental disease with 90-95% of cases attributed to environmental factors and 5-10% due to genetics.[1]Environmental, as used by cancer researchers, means any cause that is not inherited genetically, not merely pollution.[6] Common environmental factors that contribute to cancer death include tobacco (25-30%), diet and obesity (30-35%), infections (15-20%), radiation(both ionizing and non-ionizing, up to 10%), stress, lack of physical activity, and environmental pollutants.[1]It is nearly impossible to prove what caused a cancer in any individual, because most cancers have multiple possible causes. For example, if a person who uses tobacco heavily develops lung cancer, then it was probably caused by the tobacco use, but since everyone has a small chance of developing lung cancer as a result of air pollution or radiation, then there is a small chance that the cancer developed because of air pollution or radiation.
Chemicals
Further information: Alcohol and cancer and Smoking and cancerCancer pathogenesis is traceable back to DNA mutations that impact cell growth and metastasis. Substances that cause DNA mutations are known as mutagens, and mutagens that cause cancers are known as carcinogens. Particular substances have been linked to specific types of cancer. Tobacco smoking is associated with many forms of cancer,[7] and causes 90% of lung cancer.[8]
Many mutagens are also carcinogens, but some carcinogens are not mutagens. Alcohol is an example of a chemical carcinogen that is not a mutagen.[9] In Western Europe 10% of cancers in males and 3% of cancers in females are attributed to alcohol.[10]
Decades of research has demonstrated the link between tobacco use and cancer in the lung,larynx, head, neck, stomach, bladder, kidney, esophagus and pancreas.[11] Tobacco smoke contains over fifty known carcinogens, including nitrosamines and polycyclic aromatic hydrocarbons.[12] Tobacco is responsible for about one in three of all cancer deaths in the developed world,[7] and about one in five worldwide.[12] Lung cancer death rates in the United States have mirrored smoking patterns, with increases in smoking followed by dramatic increases in lung cancer death rates and, more recently, decreases in smoking rates since the 1950s followed by decreases in lung cancer death rates in men since 1990.[13][14] However, the numbers of smokers worldwide is still rising, leading to what some organizations have described as the tobacco epidemic.[15]
Cancer related to one's occupation is believed to represent between 2–20% of all cases.[16] Every year, at least 200,000 people die worldwide from cancer related to their workplace.[17] Most cancer deaths caused by occupational risk factors occur in the developed world.[17] It is estimated that approximately 20,000 cancer deaths and 40,000 new cases of cancer each year in the U.S. are attributable to occupation.[18]Millions of workers run the risk of developing cancers such as lung cancer and mesothelioma from inhaling asbestos fibers and tobacco smoke, or leukemia from exposure to benzene at their workplaces.[17]
Diet and exercise
Diet, physical inactivity, and obesity are related to approximately 30–35% of cancer deaths.[1][19] In the United States excess body weight is associated with the development of many types of cancer and is a factor in 14–20% of all cancer deaths.[19] Physical inactivity is believed to contribute to cancer risk not only through its effect on body weight but also through negative effects on immune system and endocrine system.[19]Diets that are low in vegetables, fruits and whole grains, and high in processed or red meats are linked with a number of cancers.[19] A highsalt diet is linked to gastric cancer, aflatoxin B1, a frequent food contaminate, with liver cancer, and Betel nut chewing with oral cancer.[20]This may partly explain differences in cancer incidence in different countries for example gastric cancer is more common in Japan with its high salt diet[21] and colon cancer is more common in the United States. Immigrants develop the risk of their new country, often within one generation, suggesting a substantial link between diet and cancer.[22]
Infection
Main article: Infectious causes of cancerWorldwide approximately 18% of cancer deaths are related to infectious diseases.[1] This proportion varies in different regions of the world from a high of 25% in Africa to less than 10% in the developed world.[1] Viruses are the usual infectious agents that cause cancer butbacteria and parasites may also have an effect.
A virus that can cause cancer is called an oncovirus. These include human papillomavirus (cervical carcinoma), Epstein-Barr virus (B-cell lymphoproliferative disease and nasopharyngeal carcinoma), Kaposi's sarcoma herpesvirus (Kaposi's Sarcoma and primary effusion lymphomas), hepatitis B and hepatitis C viruses (hepatocellular carcinoma), and Human T-cell leukemia virus-1 (T-cell leukemias). Bacterial infection may also increase the risk of cancer, as seen in Helicobacter pylori-induced gastric carcinoma.[23] Parasitic infections strongly associated with cancer include Schistosoma haematobium (squamous cell carcinoma of the bladder) and the liver flukes, Opisthorchis viverrini and Clonorchis sinensis (cholangiocarcinoma).[24]
Radiation
Up to 10% of invasive cancers are related to radiation exposure, including both ionizing radiation and non-ionizing radiation.[1] Additionally, the vast majority of non-invasive cancers are non-melanoma skin cancers caused by non-ionizing ultraviolet radiation.Sources of ionizing radiation include medical imaging, and radon gas. Radiation can cause cancer in most parts of the body, in all animals, and at any age, although radiation-induced solid tumors usually take 10–15 years, and can take up to 40 years, to become clinically manifest, and radiation-induced leukemias typically require 2–10 years to appear.[25] Some people, such as those with nevoid basal cell carcinoma syndrome or retinoblastoma, are more susceptible than average to developing cancer from radiation exposure.[25] Children and adolescents are twice as likely to develop radiation-induced leukemia as adults; radiation exposure before birth has ten times the effect.[25]Ionizing radiation is not a particularly strong mutagen.[25] Residential exposure to radon gas, for example, has similar cancer risks as passive smoking.[25] Low-dose exposures, such as living near a nuclear power plant, are generally believed to have no or very little effect on cancer development.[25] Radiation is a more potent source of cancer when it is combined with other cancer-causing agents, such as radon gas exposure plus smoking tobacco.[25]
Unlike chemical or physical triggers for cancer, ionizing radiation hits molecules within cells randomly. If it happens to strike a chromosome, it can break the chromosome, result in an abnormal number of chromosomes, inactivate one or more genes in the part of the chromosome that it hit, delete parts of the DNA sequence, cause chromosome translocations, or cause other types of chromosome abnormalities.[25]Major damage normally results in the cell dying, but smaller damage may leave a stable, partly functional cell that may be capable of proliferating and developing into cancer, especially if tumor suppressor genes were damaged by the radiation.[25] Three independent stages appear to be involved in the creation of cancer with ionizing radiation: morphological changes to the cell, acquiring cellular immortality (losing normal, life-limiting cell regulatory processes), and adaptations that favor formation of a tumor.[25] Even if the radiation particle does not strike the DNA directly, it triggers responses from cells that indirectly increase the likelihood of mutations.[25]
Medical use of ionizing radiation is a growing source of radiation-induced cancers. Ionizing radiation may be used to treat other cancers, but this may, in some cases, induce a second form of cancer.[25] It is also used in some kinds of medical imaging. One report estimates that approximately 29,000 future cancers could be related to the approximately 70 million CT scans performed in the US in 2007.[26] It is estimated that 0.4% of cancers in 2007 in the United States are due to CTs performed in the past and that this may increase to as high as 1.5–2% with rates of CT usage during this same time period.[27]
Prolonged exposure to ultraviolet radiation from the sun can lead to melanoma and other skin malignancies.[28] Clear evidence establishes ultraviolet radiation, especially the non-ionizing medium wave UVB, as the cause of most non-melanoma skin cancers, which are the most common forms of cancer in the world.[28]
Non-ionizing radio frequency radiation from mobile phones, electric power transmission, and other similar sources have been described as apossible carcinogen by the World Health Organization's International Agency for Research on Cancer.[29]
Heredity
Main article: Cancer syndromeThe vast majority of cancers are non-hereditary ("sporadic cancers"). Hereditary cancers are primarily caused by an inherited genetic defect. Less than 0.3% of the population are carriers of a genetic mutation which has a large effect on cancer risk and these cause less than 3–10% of all cancer.[30] Some of these syndromes include: certain inherited mutations in the genes BRCA1 and BRCA2 with a more than 75% risk of breast cancer and ovarian cancer,[30] and hereditary nonpolyposis colorectal cancer (HNPCC or Lynch syndrome) which is present in about 3% of people with colorectal cancer,[31] among others.
Physical agents
Some substances cause cancer primarily through their physical, rather than chemical, effects on cells.[32]A prominent example of this is prolonged exposure to asbestos, naturally occurring mineral fibers which are a major cause of mesothelioma, a type of lung cancer.[32] Other substances in this category, including both naturally occurring and synthetic asbestos-like fibers such aswollastonite, attapulgite, glass wool, and rock wool, are believed to have similar effects.[32]
Nonfibrous particulate materials that cause cancer include powdered metallic cobalt and nickel, and crystalline silica (quartz, cristobalite, andtridymite).[32]
Usually, physical carcinogens must get inside the body (such as through inhaling tiny pieces) and require years of exposure to develop cancer.[32]
Physical trauma resulting in cancer is relatively rare.[33] Claims that breaking bone resulted in bone cancer, for example, have never been proven.[33] Similarly, physical trauma is not accepted as a cause for cervical cancer, breast cancer, or brain cancer.[33]
One accepted source is frequent, long-term application of hot objects to the body. It is possible that repeated burns on the same part of the body, such as those produced by kanger and kairo heaters (charcoal hand warmers), may produce skin cancer, especially if carcinogenic chemicals are also present.[33] Frequently drinking scalding hot tea may produce esophageal cancer.[33]
Generally, it is believed that the cancer arises, or a pre-existing cancer is encouraged, during the process of repairing the trauma, rather than the cancer being caused directly by the trauma.[33] However, repeated injuries to the same tissues might promote excessive cell proliferation, which could then increase the odds of a cancerous mutation. There is no evidence that inflammation itself causes cancer.[33]
Hormones
Some hormones play a role in the development of cancer by promoting cell proliferation.[34] Hormones are important agents in sex-related cancers such as cancer of the breast, endometrium, prostate, ovary, and testis, and also of thyroid cancer and bone cancer.[34]An individual's hormone levels are mostly determined genetically, so this may at least partly explains the presence of some cancers that run in families that do not seem to have any cancer-causing genes.[34] For example, the daughters of women who have breast cancer have significantly higher levels of estrogen and progesterone than the daughters of women without breast cancer. These higher hormone levels may explain why these women have higher risk of breast cancer, even in the absence of a breast-cancer gene.[34] Similarly, men of African ancestry have significantly higher levels of testosterone than men of European ancestry, and have a correspondingly much higher level of prostate cancer.[34] Men of Asian ancestry, with the lowest levels of testosterone-activating androstanediol glucuronide, have the lowest levels of prostate cancer.[34]
However, non-genetic factors are also relevant: obese people have higher levels of some hormones associated with cancer and a higher rate of those cancers.[34] Women who take hormone replacement therapy have a higher risk of developing cancers associated with those hormones.[34] On the other hand, people who exercise far more than average have lower levels of these hormones, and lower risk of cancer.[34] Osteosarcoma may be promoted by growth hormones.[34] Some treatments and prevention approaches leverage this cause by artificially reducing hormone levels, and thus discouraging hormone-sensitive cancers.[34]
Other
Excepting the rare transmissions that occur with pregnancies and only a marginal few organ donors, cancer is generally not a transmissible disease. The main reason for this is tissue graft rejection caused by MHC incompatibility.[35] In humans and other vertebrates, the immune system uses MHC antigens to differentiate between "self" and "non-self" cells because these antigens are different from person to person. When non-self antigens are encountered, the immune system reacts against the appropriate cell. Such reactions may protect against tumour cell engraftment by eliminating implanted cells. In the United States, approximately 3,500 pregnant women have a malignancy annually, and transplacental transmission of acute leukaemia, lymphoma, melanoma and carcinoma from mother to fetus has been observed.[35] The development of donor-derived tumors from organ transplants is exceedingly rare. The main cause of organ transplant associated tumors seems to be malignant melanoma, that was undetected at the time of organ harvest.[36] Cancer from one organism will usually grow in another organism of that species, as long as they share the same histocompatibility genes,[37] proven using mice; however this would never happen in a real-world setting except as described above.In non-humans, a few types of transmissible cancer have been described, wherein the cancer spreads between animals by transmission of the tumor cells themselves. This phenomenon is seen in dogs with Sticker's sarcoma, also known as canine transmissible venereal tumor,[38] as well as devil facial tumour disease in Tasmanian devils.
Pathophysiology
Main article: Carcinogenesis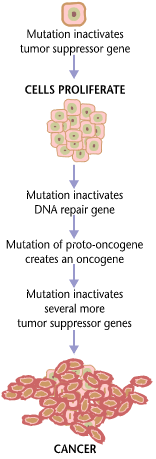

Cancers are caused by a series of mutations. Each mutation alters the behavior of the cell somewhat.
Cancer is fundamentally a disease of failure of regulation of tissue growth. In order for a normal cell totransform into a cancer cell, the genes which regulate cell growth and differentiation must be altered.[39]The affected genes are divided into two broad categories. Oncogenes are genes which promote cell growth and reproduction. Tumor suppressor genes are genes which inhibit cell division and survival. Malignant transformation can occur through the formation of novel oncogenes, the inappropriate over-expression of normal oncogenes, or by the under-expression or disabling of tumor suppressor genes. Typically, changes inmany genes are required to transform a normal cell into a cancer cell.[40]
Genetic changes can occur at different levels and by different mechanisms. The gain or loss of an entirechromosome can occur through errors in mitosis. More common are mutations, which are changes in thenucleotide sequence of genomic DNA.
Large-scale mutations involve the deletion or gain of a portion of a chromosome. Genomic amplificationoccurs when a cell gains many copies (often 20 or more) of a small chromosomal locus, usually containing one or more oncogenes and adjacent genetic material. Translocation occurs when two separate chromosomal regions become abnormally fused, often at a characteristic location. A well-known example of this is thePhiladelphia chromosome, or translocation of chromosomes 9 and 22, which occurs in chronic myelogenous leukemia, and results in production of the BCR-abl fusion protein, an oncogenic tyrosine kinase.
Small-scale mutations include point mutations, deletions, and insertions, which may occur in the promoterregion of a gene and affect its expression, or may occur in the gene's coding sequence and alter the function or stability of its protein product. Disruption of a single gene may also result from integration of genomic material from a DNA virus or retrovirus, and resulting in the expression of viral oncogenes in the affected cell and its descendants.
Replication of the enormous amount of data contained within the DNA of living cells will probabilistically result in some errors (mutations). Complex error correction and prevention is built into the process, and safeguards the cell against cancer. If significant error occurs, the damaged cell can "self-destruct" through programmed cell death, termed apoptosis. If the error control processes fail, then the mutations will survive and be passed along to daughter cells.
Some environments make errors more likely to arise and propagate. Such environments can include the presence of disruptive substances called carcinogens, repeated physical injury, heat, ionising radiation, orhypoxia[41]
The errors which cause cancer are self-amplifying and compounding, for example:
- A mutation in the error-correcting machinery of a cell might cause that cell and its children to accumulate errors more rapidly.
- A further mutation in an oncogene might cause the cell to reproduce more rapidly and more frequently than its normal counterparts.
- A further mutation may cause loss of a tumour suppressor gene, disrupting the apoptosis signalling pathway and resulting in the cell becoming immortal.
- A further mutation in signaling machinery of the cell might send error-causing signals to nearby cells.
Diagnosis
Chest x-ray showing lung cancer in the left lung.
Most cancers are initially recognized either because of the appearance of signs or symptoms or through screening. Neither of these lead to a definitive diagnosis, which requires the examination of a tissue sample by a pathologist. People with suspected cancer are investigated with medical tests. These commonly include blood tests, X-rays, CT scans and endoscopy.Classification
Further information: List of cancer types and List of oncology-related termsCancers are classified by the type of cell that the tumor cells resemble and is therefore presumed to be the origin of the tumor. These types include:
- Carcinoma: Cancers derived from epithelial cells. This group includes many of the most common cancers, particularly in the aged, and include nearly all those developing in thebreast, prostate, lung, pancreas, and colon.
- Sarcoma: Cancers arising from connective tissue (i.e. bone, cartilage, fat, nerve), each of which develop from cells originating in mesenchymal cells outside the bone marrow.
- Lymphoma and leukemia: These two classes of cancer arise from hematopoietic (blood-forming) cells that leave the marrow and tend to mature in the lymph nodes and blood, respectively.
- Germ cell tumor: Cancers derived from pluripotent cells, most often presenting in the testicle or the ovary (seminoma and dysgerminoma, respectively).
- Blastoma: Cancers derived from immature "precursor" cells or embryonic tissue. These are also most common in children.[citation needed]
Benign tumors (which are not cancers) are named using -oma as a suffix with the organ name as the root. For example, a benign tumor of smooth muscle cells is called a leiomyoma (the common name of this frequently occurring benign tumor in the uterus is fibroid). Confusingly, some types of cancer also use the -oma suffix, examples including melanoma and seminoma.
Some types of cancer are named for the size and shape of the cells under a microscope, such as giant cell carcinoma, spindle cell carcinoma, and small cell carcinoma.
Pathology
The tissue diagnosis given by the pathologist indicates the type of cell that is proliferating, its histological grade, genetic abnormalities, and other features of the tumor. Together, this information is useful to evaluate the prognosis of the patient and to choose the best treatment.Cytogenetics and immunohistochemistry are other types of testing that the pathologist may perform on the tissue specimen. These tests may provide information about the molecular changes (such as mutations, fusion genes, and numerical chromosome changes) that has happened in the cancer cells, and may thus also indicate the future behavior of the cancer (prognosis) and best treatment.- An invasive ductal carcinoma of the breast (pale area at the center) surrounded by spikes of whitish scar tissue and yellow fatty tissue.
Prevention
Cancer prevention is defined as active measures to decrease the risk of cancer.[43] The vast majority of cancer risk factors are due to environmental (including lifestyle) factors, and many of these factors are controllable. Thus, cancer is largely considered a preventable disease.[44] Greater than 30% of cancer is considered preventable by avoiding risk factors including: tobacco, overweight / obesity, an insufficient diet, physical inactivity, alcohol, sexually transmitted infections, and air pollution.[45] Not all environmental causes can be prevented completely such as naturally occurring background radiation.Dietary
Main article: Diet and cancerWhile many dietary recommendations have been proposed to reduce the risk of cancer, few have significant supporting scientific evidence.[46]The primary dietary factors that increase risk are obesity and alcohol consumption; with a diet low in fruits and vegetables and high in red meat being implicated but not confirmed.[47][48] Consumption of coffee is associated with a reduced risk of liver cancer.[49] Studies have linked consumption of red or processed meat to an increased risk of breast cancer, colon cancer, and pancreatic cancer, a phenomenon which could be due to the presence of carcinogens in foods cooked at high temperatures.[50][51] Thus dietary recommendation for cancer prevention typically include: "mainly vegetables, fruit, whole grain and fish and a reduced intake of red meat, animal fat and refined sugar."[46]
Medication
The concept that medications can be used to prevent cancer is attractive, and evidence supports their use in a few defined circumstances.[52]In the general population NSAIDs reduce the risk of colorectal cancer however due to the cardiovascular and gastrointestinal side effects they cause overall harm when used for prevention.[53] Aspirin has been found to reduce the risk of death from cancer by about 7%.[54] COX-2 inhibitor may decrease the rate of polyp formation in people with familial adenomatous polyposis however are associated with the same adverse effects as NSAIDs.[55] Daily use of tamoxifen or raloxifene has been demonstrated to reduce the risk of developing breast cancer in high-risk women.[56] The benefit verses harm for 5-alpha-reductase inhibitor such as finasteride is not clear.[57]Vitamins have not been found to be effective at preventing cancer,[58] although low blood levels of vitamin D are correlated with increased cancer risk.[59][60] Whether this relationship is causal and vitamin D supplementation is protective is not determined.[61] Beta-carotenesupplementation has been found to increase lung cancer rates in those who are high risk.[62] Folic acid supplementation has not been found effective in preventing colon cancer and may increase colon polyps.[63]
Vaccination
Vaccines have been developed that prevent some infection by some viruses.[64] Human papillomavirus vaccine (Gardasil and Cervarix) decreases the risk of developing cervical cancer.[64] The hepatitis B vaccine prevents infection with hepatitis B virus and thus decreases the risk of liver cancer.[64]Screening
Main article: Cancer screeningUnlike diagnosis efforts prompted by symptoms and medical signs, cancer screening involves efforts to detect cancer after it has formed, but before any noticeable symptoms appear.[65] This may involve physical examination, blood or urine tests, or medical imaging.[65]
Cancer screening is currently not possible for many types of cancers, and even when tests are available, they may not be recommended for everyone. Universal screening or mass screening involves screening everyone.[66] Selective screening identifies people who are known to be at higher risk of developing cancer, such as people with a family history of cancer.[66] Several factors are considered to determine whether the benefits of screening outweigh the risks and the costs of screening.[65] These factors include:
- Possible harms from the screening test: for example, X-ray images involve exposure to potentially harmful ionizing radiation.
- The likelihood of the test correctly identifying cancer.
- The likelihood of cancer being present: Screening is not normally useful for rare cancers.
- Possible harms from follow-up procedures.
- Whether suitable treatment is available.
- Whether early detection improves treatment outcomes.
- Whether the cancer will ever need treatment.
- Whether the test is acceptable to the people: If a screening test is too burdensome (for example, being extremely painful), then people will refuse to participate.[66]
- Cost of the test.
Recommendations
The U.S. Preventive Services Task Force (USPSTF) strongly recommends cervical cancer screening in women who are sexually active and have a cervix at least until the age of 65.[67] They recommend that Americans be screened for colorectal cancer via fecal occult blood testing,sigmoidoscopy, or colonoscopy starting at age 50 until age 75.[68] There is insufficient evidence to recommend for or against screening forskin cancer,[69] oral cancer,[70] lung cancer,[71] or prostate cancer in men under 75.[72] Routine screening is not recommended for bladder cancer,[73] testicular cancer,[74] ovarian cancer,[75] pancreatic cancer,[76] or prostate cancer.[77]The USPSTF recommends mammography for breast cancer screening every two years for those 50–74 years old; however, they do not recommend either breast self-examination or clinical breast examination.[78] A 2011 Cochrane review came to slightly different conclusions with respect to breast cancer screening stating that routine mammography may do more harm than good.[79]
Japan screens for gastric cancer using photofluorography due to the high incidence there.[3]
Genetic testing
See also: Cancer syndrome| Gene | Cancer types |
| Breast, ovarian, pancreatic | |
| Colon, uterine, small bowel, stomach, urinary tract |
Genetic testing for individuals at high-risk of certain cancers is recommended.[80] Carriers of these mutations may than undergo enhanced surveillance, chemoprevention, or preventative surgery to reduce their subsequent risk.[80]
Management
Main article: Management of cancerMany management options for cancer exist with the primary ones including: surgery, chemotherapy, radiation therapy, and palliative care. Which treatments are used depends upon the type, location and grade of the cancer as well as the person's health and wishes.
Surgery
Surgery is the primary method of treatment of most isolated solid cancers and may play a role in palliation and prolongation of survival. It is typically an important part of making the definitive diagnosis and staging the tumor as biopsies are usually required. In localized cancer surgery typically attempts to remove the entire mass along with, in certain cases, the lymph nodes in the area. For some types of cancer this is all that is needed for a good outcome.[81]Chemotherapy
Chemotherapy in addition to surgery has proven useful in a number of different cancer types including: breast cancer, colorectal cancer,pancreatic cancer, osteogenic sarcoma, testicular cancer, ovarian cancer, and certain lung cancers.[81] The effectiveness of chemotherapy is often limited by toxicity to other tissues in the body.Radiation
Radiation therapy involves the use of ionizing radiation in an attempt to either cure or improve the symptoms of cancer. It is used in about half of all cases and the radiation can be from either internal sources in the form of brachytherapy or external sources. Radiation is typically used in addition to surgery and or chemotherapy but for certain types of cancer such as early head and neck cancer may be used alone. For painful bone metastasis it has been found to be effective in about 70% of people.[82]Alternative treatments
Complementary and alternative cancer treatments are a diverse group of health care systems, practices, and products that are not part of conventional medicine and have not been shown to be effective.[83] "Complementary medicine" refers to methods and substances used along with conventional medicine, while "alternative medicine" refers to compounds used instead of conventional medicine.[84] Most complementary and alternative medicines for cancer have not been rigorously studied or tested. Some alternative treatments have been investigated and shown to be ineffective but still continue to be marketed and promoted.[85]Palliative care
Palliative care is an approach to symptom management that aims to reduce the physical, emotional, spiritual, and psycho-social distress experienced by people with cancer. Unlike treatment that is aimed at directly killing cancer cells, the primary goal of palliative care is to make the person feel better.Palliative care is often confused with hospice and therefore only involved when people approach end of life. Like hospice care, palliative care attempts to help the person cope with the immediate needs and to increase the person's comfort. Unlike hospice care, palliative care does not require people to stop treatment aimed at prolonging their lives or curing the cancer.
Multiple national medical guidelines recommend early palliative care for people whose cancer has produced distressing symptoms (pain, shortness of breath, fatigue, nausea) or who need help coping with their illness. In people who have metastatic disease when first diagnosed, oncologists should consider a palliative care consult immediately. Additionally, an oncologist should consider a palliative care consult in any patient they feel has a prognosis of less than 12 months even if continuing aggressive treatment.[86][87][88]
Prognosis
See also: Cancer survivorCancer has a reputation as a deadly disease. Taken as a whole, about half of people receiving treatment for invasive cancer (excludingcarcinoma in situ and non-melanoma skin cancers) die from cancer or its treatment.[3] Survival is worse in the developing world.[3] However, the survival rates vary dramatically by type of cancer, with the range running from basically all people surviving to almost no one surviving.
Those who survive cancer are at increased risk of developing a second primary cancer at about twice the rate of those never diagnosed with cancer.[89] The increased risk is believed to be primarily due to the same risk factors that produced the first cancer, partly due to the treatment for the first cancer, and potentially related to better compliance with screening.[89]
Predicting either short-term or long-term survival is difficult and depends on many factors. The most important factors are the particular kind of cancer and the patient's age and overall health. People who are frail with many other health problems have lower survival rates than otherwise healthy people. A centenarian is unlikely to survive for five years even if the treatment is successful. People who report a higher quality of life tend to survive longer.[90] People with lower quality of life may be affected by major depressive disorder and other complications from cancer treatment and/or disease progression that both impairs their quality of life and reduces their quantity of life. Additionally, patients with worse prognoses may be depressed or report a lower quality of life directly because they correctly perceive that their condition is likely to be fatal.
In 2007, the overall costs of cancer in the U.S. — including treatment and indirect mortality expenses (such as lost productivity in the workplace) — was estimated to be $226.8 billion. In 2009, 32% of Hispanics and 10% of children 17 years old or younger lacked health insurance; "uninsured patients and those from ethnic minorities are substantially more likely to be diagnosed with cancer at a later stage, when treatment can be more extensive and more costly."[91]
Epidemiology
Main article: Epidemiology of cancerDeath rate from malignant cancer per 100,000 inhabitants in 2004.[92]
| no data ≤ 55 55-80 80-105 105-130 130-155 155-180 | 180-205 205-230 230-255 255-280 280-305 ≥ 305 |
In 2008 approximately 12.7 million cancers were diagnosed (excluding non-melanoma skin cancers and other non-invasive cancers) and 7.6 million people died of cancer worldwide.[3]Cancers as a group account for approximately 13% of all deaths each year with the most common being: lung cancer (1.4 million deaths), stomach cancer (740,000 deaths), liver cancer (700,000 deaths), colorectal cancer (610,000 deaths), and breast cancer (460,000 deaths).[93] This makes invasive cancer the leading cause of death in the developed world and the second leading cause of death in the developing world.[3] Over half of cases occur in the developing world.[3]
Global cancer rates have been increasing primarily due to an aging population and lifestyle changes in the developing world.[3] The most significant risk factor for developing cancer is old age.[94] Although it is possible for cancer to strike at any age, most people who are diagnosed with invasive cancer are over the age of 65.[94] According to cancer researcher Robert A. Weinberg, "If we lived long enough, sooner or later we all would get cancer."[95] Some of the association between aging and cancer is attributed to immunosenescence,[96] errors accumulated in DNA over a lifetime, and age-related changes in the endocrine system.[97]
Some slow-growing cancers are particularly common. Autopsy studies in Europe and Asia have shown that up to 36% of people have undiagnosed and apparently harmless thyroid cancer at the time of their deaths, and that 80% of men develop prostate cancer by age 80.[98][99] As these cancers did not cause the person's death, identifying them would have represented overdiagnosis rather than useful medical care.
The three most common childhood cancers are leukemia (34%), brain tumors (23%), and lymphomas (12%).[100] Rates of childhood cancer have increased by 0.6% per year between 1975 to 2002 in the United States[101] and by 1.1% per year between 1978 and 1997 in Europe.[100]
History
Main article: History of cancerEngraving with two views of a Dutch woman who had a tumor removed from her neck in 1689.
The earliest written record regarding cancer is from 3000 BC in the Egyptian Edwin Smith Papyrusand describes cancer of the breast.[102] Cancer however has existed for all of human history.[102]Hippocrates (ca. 460 BC – ca. 370 BC) described several kinds of cancer, referring to them with the Greek word carcinos (crab or crayfish).[102] This name comes from the appearance of the cut surface of a solid malignant tumour, with "the veins stretched on all sides as the animal the crab has its feet, whence it derives its name".[103] The Greek, Celsus (ca. 25 BC - 50 AD) translatedcarcinos into the Latin cancer, also meaning crab and recommended surgery as treatment.[102]Galen (2nd century AD) disagreed with the use of surgery and recommended purgativesinstead.[102] These recommendations largely stood for 1000 years.[102]In the 15th, 16th and 17th centuries, it became more acceptable for doctors to dissect bodies to discover the cause of death.[104] The German professor Wilhelm Fabry believed that breast cancer was caused by a milk clot in a mammary duct. The Dutch professor Francois de la Boe Sylvius, a follower of Descartes, believed that all disease was the outcome of chemical processes, and that acidic lymph fluid was the cause of cancer. His contemporary Nicolaes Tulp believed that cancer was a poison that slowly spreads, and concluded that it was contagious.[105]
The physician John Hill described tobacco snuff as the cause of nose cancer in 1761.[104] This was followed by the report in 1775 by British surgeon Percivall Pott that cancer of the scrotum was a common disease among chimney sweeps.[106] With the widespread use of the microscope in the 18th century, it was discovered that the 'cancer poison' spread from the primary tumor through the lymph nodes to other sites ("metastasis"). This view of the disease was first formulated by the English surgeon Campbell De Morgan between 1871 and 1874.[107]
Society and culture
Though many diseases (such as heart failure) may have a worse prognosis than most cases of cancer, cancer is the subject of widespread fear and taboos. The euphemism, "after a long illness" is still commonly used (2012) reflecting an apparent stigma.[108] This deep belief that cancer is necessarily a difficult and usually deadly disease is reflected in the systems chosen by society to compile cancer statistics: the most common form of cancer—non-melanoma skin cancers, accounting for about one-third of all cancer cases worldwide, but very few deaths[109][110]—are excluded from cancer statistics specifically because they are easily treated and almost always cured, often in a single, short, outpatient procedure.[111]Cancer is regarded as a disease that must be "fought" to end the "civil insurrection"; a War on Cancer has been declared. Military metaphors are particularly common in descriptions of cancer's human effects, and they emphasize both the parlous state of the affected individual's health and the need for the individual to take immediate, decisive actions himself, rather than to delay, to ignore, or to rely entirely on others caring for him. The military metaphors also help rationalize radical, destructive treatments.[112][113]
In the 1970s, a relatively popular alternative cancer treatment was a specialized form of talk therapy, based on the idea that cancer was caused by a bad attitude.[114] People with a "cancer personality"—depressed, repressed, self-loathing, and afraid to express their emotions—were believed to have manifested cancer through subconscious desire. Some psychotherapists said that treatment to change the patient's outlook on life would cure the cancer.[114] Among other effects, this belief allows society to blame the victim for having caused the cancer (by "wanting" it) or having prevented its cure (by not becoming a sufficiently happy, fearless, and loving person).[115] It also increases patients' anxiety, as they incorrectly believe that natural emotions of sadness, anger or fear shorten their lives.[115] The idea was excoriated by the notoriously outspoken Susan Sontag, who published Illness as Metaphor while recovering from treatment for breast cancer in 1978.[114]Although the original idea is now generally regarded as nonsense, the idea partly persists in a reduced form with a widespread, but incorrect, belief that deliberately cultivating a habit of positive thinking will increase survival.[115] This notion is particularly strong in breast cancer culture.[115]
Research
Main article: Cancer researchBecause cancer is a class of diseases,[116][117] it is unlikely that there will ever be a single "cure for cancer" any more than there will be a single treatment for all infectious diseases.[118] Angiogenesis inhibitors were once thought to have potential as a "silver bullet" treatment applicable to many types of cancer, but this has not been the case in practice.[119]
Experimental cancer treatments are treatments that are being studied to see whether they work. Typically, these are studied in clinical trialsto compare the proposed treatment to the best existing treatment. They may be entirely new treatments, or they may be treatments that have been used successfully in one type of cancer, and are now being tested to see whether they are effective in another type.[120] More and more, such treatments are being developed alongside companion diagnostic tests to target the right drugs to the right patients, based on their individual biology.[121]
Cancer research is the intense scientific effort to understand disease processes and discover possible therapies.
Research about cancer causes focuses on the following issues:
- Agents (e.g. viruses) and events (e.g. mutations) which cause or facilitate genetic changes in cells destined to become cancer.
- The precise nature of the genetic damage, and the genes which are affected by it.
- The consequences of those genetic changes on the biology of the cell, both in generating the defining properties of a cancer cell, and in facilitating additional genetic events which lead to further progression of the cancer.
In pregnancy
Because cancer is largely a disease of older adults, it is not common in pregnant women. Cancer affects approximately 1 in 1,000 pregnant women.[124] The most common cancers found during pregnancy are the same as the most common cancers found in non-pregnant women during childbearing ages: breast cancer, cervical cancer, leukemia, lymphoma, melanoma, ovarian cancer, and colorectal cancer.[124]Diagnosing a new cancer in a pregnant woman is difficult, in part because any symptoms are commonly assumed to be a normal discomfort associated with pregnancy.[124] As a result, cancer is typically discovered at a somewhat later stage than average in many pregnant or recently pregnant women. Some imaging procedures, such as MRIs (magnetic resonance imaging), CT scans, ultrasounds, andmammograms with fetal shielding are considered safe during pregnancy; some others, such as PET scans are not.[124]
Treatment is generally the same as for non-pregnant women.[124] However, radiation and radioactive drugs are normally avoided during pregnancy, especially if the fetal dose might exceed 100 cGy. In some cases, some or all treatments are postponed until after birth if the cancer is diagnosed late in the pregnancy. Early deliveries to speed the start of treatment are not uncommon. Surgery is generally safe, but pelvic surgeries during the first trimester may cause miscarriage. Some treatments, especially certain chemotherapy drugs given during thefirst trimester, increase the risk of birth defects and pregnancy loss (spontaneous abortions and stillbirths).[124]
Elective abortions are not required and, for the most common forms and stages of cancer, do not improve the likelihood of the mother surviving or being cured.[124] In a few instances, such as advanced uterine cancer, the pregnancy cannot be continued, and in others, such as an acute leukemia discovered early in pregnancy, the pregnant woman may choose to have abortion so that she can begin aggressive chemotherapy without worrying about birth defects.[124]
Some treatments may interfere with the mother's ability to give birth vaginally or to breastfeed her baby.[124] Cervical cancer may require birth by Caesarean section. Radiation to the breast reduces the ability of that breast to produce milk and increases the risk of mastitis. Also, when chemotherapy is being given after birth, many of the drugs pass through breast milk to the baby, which could harm the baby.[124]
Notes
- ^ a b c d e f g Anand P, Kunnumakkara AB, Kunnumakara AB, et al.(September 2008). "Cancer is a Preventable Disease that Requires Major Lifestyle Changes". Pharm. Res. 25 (9): 2097–116. doi:10.1007/s11095-008-9661-9. PMC 2515569.PMID 18626751.
- ^ Kinzler, Kenneth W.; Vogelstein, Bert (2002). "Introduction". The genetic basis of human cancer (2nd, illustrated, revised ed.). New York: McGraw-Hill, Medical Pub. Division. p. 5. ISBN 978-0-07-137050-9.
- ^ a b c d e f g h Jemal, A; Bray, F, Center, MM, Ferlay, J, Ward, E, Forman, D (2011-02-04). "Global cancer statistics". CA: a cancer journal for clinicians 61 (2): 69–90. doi:10.3322/caac.20107.PMID 21296855.
- ^ a b c d e Holland Chp. 1
- ^ O'Dell, edited by Michael D. Stubblefield, Michael W. (2009).Cancer rehabilitation principles and practice. New York: Demos Medical. pp. 983. ISBN 978-1-933864-33-4.
- ^ Julia Kravchenko; Igor Akushevich; Manton, Kenneth G. (2009).Cancer mortality and morbidity patterns in the U. S. population: an interdisciplinary approach. Berlin: Springer. p. 118. ISBN 0-387-78192-7. "The term environment refers not only to air, water, and soil but also to substances and conditions at home and at the workplace, including diet, smoking, alcohol, drugs, exposure to chemicals, sunlight, ionizing radiation, electromagnetic fields, infectious agents, etc. Lifestyle, economic and behavioral factors are all aspects of our environment."
- ^ a b Sasco AJ, Secretan MB, Straif K (August 2004). "Tobacco smoking and cancer: a brief review of recent epidemiological evidence". Lung cancer (Amsterdam, Netherlands) 45 Suppl 2: S3–9. doi:10.1016/j.lungcan.2004.07.998. PMID 15552776.
- ^ Biesalski HK, Bueno de Mesquita B, Chesson A, et al. (1998)."European Consensus Statement on Lung Cancer: risk factors and prevention. Lung Cancer Panel". CA: a cancer journal for clinicians 48 (3): 167–76; discussion 164–6.doi:10.3322/canjclin.48.3.167. PMID 9594919.
- ^ Seitz HK, Pöschl G, Simanowski UA (1998). "Alcohol and cancer".Recent developments in alcoholism : an official publication of the American Medical Society on Alcoholism, the Research Society on Alcoholism, and the National Council on Alcoholism 14: 67–95.PMID 9751943.
- ^ Schütze, M; Boeing, H, Pischon, T, Rehm, J, Kehoe, T, Gmel, G, Olsen, A, Tjønneland, AM, Dahm, CC, Overvad, K, Clavel-Chapelon, F, Boutron-Ruault, MC, Trichopoulou, A, Benetou, V, Zylis, D, Kaaks, R, Rohrmann, S, Palli, D, Berrino, F, Tumino, R, Vineis, P, Rodríguez, L, Agudo, A, Sánchez, MJ, Dorronsoro, M, Chirlaque, MD, Barricarte, A, Peeters, PH, van Gils, CH, Khaw, KT, Wareham, N, Allen, NE, Key, TJ, Boffetta, P, Slimani, N, Jenab, M, Romaguera, D, Wark, PA, Riboli, E, Bergmann, MM (2011-04-07). "Alcohol attributable burden of incidence of cancer in eight European countries based on results from prospective cohort study". BMJ (Clinical research ed.) 342: d1584. doi:10.1136/bmj.d1584.PMC 3072472. PMID 21474525.
- ^ Kuper H, Boffetta P, Adami HO (September 2002). "Tobacco use and cancer causation: association by tumour type". Journal of internal medicine 252 (3): 206–24. doi:10.1046/j.1365-2796.2002.01022.x. PMID 12270001.
- ^ a b Kuper H, Adami HO, Boffetta P (June 2002). "Tobacco use, cancer causation and public health impact". Journal of internal medicine 251 (6): 455–66. doi:10.1046/j.1365-2796.2002.00993.x. PMID 12028500.
- ^ Thun, M. J (1 October 2006). "How much of the decrease in cancer death rates in the United States is attributable to reductions in tobacco smoking?". Tobacco Control 15 (5): 345–347.doi:10.1136/tc.2006.017749.
- ^ Dubey, S; Powell, CA (2008-05-01). "Update in lung cancer 2007.". American journal of respiratory and critical care medicine177 (9): 941–6. PMID 18434333.
- ^ Proctor RN (May 2004). "The global smoking epidemic: a history and status report". Clinical lung cancer 5 (6): 371–6.doi:10.3816/CLC.2004.n.016. PMID 15217537.
- ^ Irigaray P, Newby JA, Clapp R, et al. (December 2007). "Lifestyle-related factors and environmental agents causing cancer: an overview". Biomed. Pharmacother. 61 (10): 640–58.doi:10.1016/j.biopha.2007.10.006. PMID 18055160.
- ^ a b c "WHO calls for prevention of cancer through healthy workplaces" (Press release). World Health Organization. 2007-04-27. Retrieved 2007-10-13.
- ^ "National Institute for Occupational Safety and Health- Occupational Cancer". United States National Institute for Occupational Safety and Health. Retrieved 2007-10-13.
- ^ a b c d Kushi LH, Byers T, Doyle C, et al. (2006). "American Cancer Society Guidelines on Nutrition and Physical Activity for cancer prevention: reducing the risk of cancer with healthy food choices and physical activity". CA Cancer J Clin 56 (5): 254–81.doi:10.3322/canjclin.56.5.254. PMID 17005596.
- ^ Park, S; Bae, J, Nam, BH, Yoo, KY (2008 Jul-Sep). "Aetiology of cancer in Asia" (PDF). Asian Pacific journal of cancer prevention9 (3): 371–80. PMID 18990005.
- ^ Brenner, H; Rothenbacher, D, Arndt, V (2009). "Epidemiology of stomach cancer". Methods in molecular biology (Clifton, N.J.). Methods in Molecular Biology 472: 467–77. doi:10.1007/978-1-60327-492-0_23. ISBN 978-1-60327-491-3. PMID 19107449.
- ^ Buell P, Dunn JE (1965). "Cancer mortality among Japanese Issei and Nisei of California". Cancer 18 (5): 656–64.doi:10.1002/1097-0142(196505)18:5<656::AID-CNCR2820180515>3.0.CO;2-3. PMID 14278899.
- ^ Pagano JS, Blaser M, Buendia MA, et al. (December 2004). "Infectious agents and cancer: criteria for a causal relation". Semin. Cancer Biol. 14 (6): 453–71.doi:10.1016/j.semcancer.2004.06.009. PMID 15489139.
- ^ Samaras, Vassilis; Rafailidis, Petros I.; Mourtzoukou, Eleni G.; Peppas, George; Falagas, Matthew E. (May 2010). "Chronic bacterial and parasitic infections and cancer: a review" (PDF).The Journal of Infection in Developing Countries 4 (5): 267–281.ISSN 1972-2680. PMID 20539059.
- ^ a b c d e f g h i j k l Little, John B (2000). "Chapter 14: Ionizing Radiation". In Bast RC, Kufe DW, Pollock RE, et al.. Holland-Frei Cancer Medicine (5th ed.). Hamilton, Ontario: B.C. Decker. ISBN 1-55009-113-1. Retrieved 31 January 2011.
- ^ Berrington de González A, Mahesh M, Kim KP, et al. (December 2009). "Projected cancer risks from computed tomographic scans performed in the United States in 2007". Arch. Intern. Med. 169(22): 2071–7. doi:10.1001/archinternmed.2009.440.PMID 20008689.
- ^ Brenner DJ, Hall EJ (November 2007). "Computed tomography--an increasing source of radiation exposure" (PDF). N. Engl. J. Med. 357 (22): 2277–84. doi:10.1056/NEJMra072149.PMID 18046031.
- ^ a b Cleaver, James E and David L Mitchell (2000). "15. Ultraviolet Radiation Carcinogenesis". In Bast RC, Kufe DW, Pollock RE, et al.. Holland-Frei Cancer Medicine (5th ed.). Hamilton, Ontario: B.C. Decker. ISBN 1-55009-113-1. Retrieved 31 January 2011.
- ^ "IARC classifies radiofrequency electromagnetic fields as possibly carcinogenic to humans". World Health Organization.
- ^ a b Roukos, DH (2009 Apr). "Genome-wide association studies: how predictable is a person's cancer risk?" (PDF). Expert review of anticancer therapy 9 (4): 389–92. doi:10.1586/era.09.12.PMID 19374592.
- ^ Cunningham, D; Atkin, W, Lenz, HJ, Lynch, HT, Minsky, B, Nordlinger, B, Starling, N (2010-03-20). "Colorectal cancer.".Lancet 375 (9719): 1030–47. doi:10.1016/S0140-6736(10)60353-4. PMID 20304247.
- ^ a b c d e Maltoni, Cesare Franco Minardi, and James F Holland (2000). "Chapter 16: Physical Carcinogens". In Bast RC, Kufe DW, Pollock RE, et al.. Holland-Frei Cancer Medicine (5th ed.). Hamilton, Ontario: B.C. Decker. ISBN 1-55009-113-1. Retrieved 31 January 2011.
- ^ a b c d e f g Gaeta, John F (2000). "Chapter 17: Trauma and Inflammation". In Bast RC, Kufe DW, Pollock RE, et al.. Holland-Frei Cancer Medicine (5th ed.). Hamilton, Ontario: B.C. Decker.ISBN 1-55009-113-1. Retrieved 27 January 2011.
- ^ a b c d e f g h i j k Henderson, Brian E, Leslie Bernstein, and Ronald K Ross (2000). "Chapter 13: Hormones and the Etiology of Cancer". In Bast RC, Kufe DW, Pollock RE, et al.. Holland-Frei Cancer Medicine (5th ed.). Hamilton, Ontario: B.C. Decker. ISBN 1-55009-113-1. Retrieved 27 January 2011.
- ^ a b Tolar J, Neglia JP (June 2003). "Transplacental and other routes of cancer transmission between individuals". J Pediatr Hematol Oncol. 25 (6): 430–4. doi:10.1097/00043426-200306000-00002. PMID 12794519.
- ^ Dingli D, Nowak MA (September 2006). "Infectious Cancer Cells". Nature 443 (7107): 35–6. Bibcode2006Natur.443...35D. doi:10.1038/443035a. PMC 2711443.PMID 16957717.
- ^ "The Nobel Prize in Physiology or Medicine 1980".
- ^ Murgia C, Pritchard JK, Kim SY, Fassati A, Weiss RA (2006)."Clonal Origin and Evolution of a Transmissible Cancer". Cell126 (3): 477–87. doi:10.1016/j.cell.2006.05.051.PMC 2593932. PMID 16901782.
- ^ Croce CM (January 2008). "Oncogenes and cancer" (PDF).The New England journal of medicine 358 (5): 502–11.doi:10.1056/NEJMra072367. PMID 18234754.
- ^ Knudson AG (November 2001). "Two genetic hits (more or less) to cancer". Nature reviews. Cancer 1 (2): 157–62.doi:10.1038/35101031. PMID 11905807.
- ^ Nelson DA, Tan TT, Rabson AB, Anderson D, Degenhardt K, White E (September 2004). "Hypoxia and defective apoptosis drive genomic instability and tumorigenesis". Genes & Development18 (17): 2095–107. doi:10.1101/gad.1204904. PMC 515288.PMID 15314031.
- ^ Merlo LM, Pepper JW, Reid BJ, Maley CC (December 2006). "Cancer as an evolutionary and ecological process". Nat. Rev. Cancer 6 (12): 924–35. doi:10.1038/nrc2013. PMID 17109012.
- ^ "Cancer prevention: 7 steps to reduce your risk". Mayo Clinic. 2008-09-27. Retrieved 2010-01-30.
- ^ Danaei G, Vander Hoorn S, Lopez AD, Murray CJ, Ezzati M (2005). "Causes of cancer in the world: comparative risk assessment of nine behavioural and environmental risk factors". Lancet 366(9499): 1784–93. doi:10.1016/S0140-6736(05)67725-2.PMID 16298215.
- ^ "Cancer". World Health Organization. Retrieved 2011-01-09.
- ^ a b Wicki, A; Hagmann, J (2011-09-09). "Diet and cancer.". Swiss medical weekly 141: w13250. doi:10.4414/smw.2011.13250.PMID 21904992.
- ^ Cappellani, A; Di Vita, M, Zanghi, A, Cavallaro, A, Piccolo, G, Veroux, M, Berretta, M, Malaguarnera, M, Canzonieri, V, Lo Menzo, E (2012-01-01). "Diet, obesity and breast cancer: an update.".Frontiers in bioscience (Scholar edition) 4: 90–108.PMID 22202045.
- ^ Key, TJ (2011-01-04). "Fruit and vegetables and cancer risk.".British journal of cancer 104 (1): 6–11.doi:10.1038/sj.bjc.6606032. PMC 3039795.PMID 21119663.
- ^ Larsson SC, Wolk A (2007). "Coffee consumption and risk of liver cancer: a meta-analysis". Gastroenterology 132 (5): 1740–5.doi:10.1053/j.gastro.2007.03.044. PMID 17484871.
- ^ Zheng, W; Lee, SA (2009). "Well-done meat intake, heterocyclic amine exposure, and cancer risk.". Nutrition and cancer 61 (4): 437–46. doi:10.1080/01635580802710741. PMC 2769029.PMID 19838915.
- ^ Ferguson, LR (2010 Feb). "Meat and cancer.". Meat science 84(2): 308–13. doi:10.1016/j.meatsci.2009.06.032.PMID 20374790.
- ^ Holland Chp.33
- ^ Rostom, A; Dubé, C, Lewin, G, Tsertsvadze, A, Barrowman, N, Code, C, Sampson, M, Moher, D, U.S. Preventive Services Task, Force (2007-03-06). "Nonsteroidal anti-inflammatory drugs and cyclooxygenase-2 inhibitors for primary prevention of colorectal cancer: a systematic review prepared for the U.S. Preventive Services Task Force.". Annals of internal medicine 146 (5): 376–89. PMID 17339623.
- ^ Rothwell PM, Fowkes FG, Belch JF, Ogawa H, Warlow CP, Meade TW (January 2011). "Effect of daily aspirin on long-term risk of death due to cancer: analysis of individual patient data from randomised trials". Lancet 377 (9759): 31–41. doi:10.1016/S0140-6736(10)62110-1. PMID 21144578.
- ^ Cooper, K; Squires, H, Carroll, C, Papaioannou, D, Booth, A, Logan, RF, Maguire, C, Hind, D, Tappenden, P (2010 Jun). "Chemoprevention of colorectal cancer: systematic review and economic evaluation.". Health technology assessment (Winchester, England) 14 (32): 1–206. doi:10.3310/hta14320.PMID 20594533.
- ^ Thomsen, A; Kolesar, JM (2008-12-01). "Chemoprevention of breast cancer.". American journal of health-system pharmacy : AJHP : official journal of the American Society of Health-System Pharmacists 65 (23): 2221–8. doi:10.2146/ajhp070663.PMID 19020189.
- ^ Wilt, TJ; MacDonald, R, Hagerty, K, Schellhammer, P, Kramer, BS (2008-04-16). "Five-alpha-reductase Inhibitors for prostate cancer prevention.". Cochrane database of systematic reviews (Online) (2): CD007091. doi:10.1002/14651858.CD007091.PMID 18425978.
- ^ "Vitamins and minerals: not for cancer or cardiovascular prevention". Prescrire Int 19 (108): 182. August 2010.PMID 20939459.
- ^ Giovannucci E, Liu Y, Rimm EB, et al. (April 2006). "Prospective study of predictors of vitamin D status and cancer incidence and mortality in men". J. Natl. Cancer Inst. 98 (7): 451–9.doi:10.1093/jnci/djj101. PMID 16595781.
- ^ "Vitamin D Has Role in Colon Cancer Prevention". Archived from the original on December 4, 2006. Retrieved 2007-07-27.
- ^ Schwartz GG, Blot WJ (April 2006). "Vitamin D status and cancer incidence and mortality: something new under the sun". J. Natl. Cancer Inst. 98 (7): 428–30. doi:10.1093/jnci/djj127.PMID 16595770.
- ^ Fritz, H; Kennedy, D, Fergusson, D, Fernandes, R, Doucette, S, Cooley, K, Seely, A, Sagar, S, Wong, R, Seely, D (2011). "Vitamin A and retinoid derivatives for lung cancer: a systematic review and meta analysis.". PloS one 6 (6): e21107. PMID 21738614.
- ^ Cole BF, Baron JA, Sandler RS, et al. (2007). "Folic acid for the prevention of colorectal adenomas: a randomized clinical trial".Journal of the American Medical Association 297 (21): 2351–9.doi:10.1001/jama.297.21.2351. PMID 17551129.
- ^ a b c "Cancer Vaccine Fact Sheet". NCI. 2006-06-08. Retrieved 2008-11-15.
- ^ a b c "What Is Cancer Screening?". National Cancer Institute.
- ^ a b c Wilson JMG, Jungner G. (1968) Principles and practice of screening for disease. Geneva:World Health Organization. Public Health Papers, #34.
- ^ "Screening for Cervical Cancer". U.S. Preventive Services Task Force. 2003.
- ^ "Screening for Colorectal Cancer". U.S. Preventive Services Task Force. 2008.
- ^ "Screening for Skin Cancer". U.S. Preventive Services Task Force. 2009.
- ^ "Screening for Oral Cancer". U.S. Preventive Services Task Force. 2004.
- ^ "Lung Cancer Screening". U.S. Preventive Services Task Force. 2004.
- ^ "Screening for Prostate Cancer". U.S. Preventive Services Task Force. 2008.
- ^ "Screening for Bladder Cancer". U.S. Preventive Services Task Force. 2004.
- ^ "Screening for Testicular Cancer". U.S. Preventive Services Task Force. 2004.
- ^ "Screening for Ovarian Cancer". U.S. Preventive Services Task Force. 2004.
- ^ "Screening for Pancreatic Cancer". U.S. Preventive Services Task Force. 2004.
- ^ Chou, MD, Roger; Croswell, MD, MPH, Jennifer M.; Dana, MLS, Tracy; Bougatous, BS, Christina; Blazina, MPH, Ian; Fu, PhD, Rongwei; Gleitsmann, MD, MPH, Ken; Koenig, MD, MPH, Helen C. et al (7 October 2011). "Screening for Prostate Cancer - A Review of the Evidence for the U.S. Preventive Services Task Force".United States Preventive Services Task Force. Retrieved 2011-10-08.
- ^ "Screening for Breast Cancer". U.S. Preventive Services Task Force. 2009.
- ^ Gøtzsche PC, Nielsen M (2011). "Screening for breast cancer with mammography". Cochrane Database Syst Rev (1): CD001877. doi:10.1002/14651858.CD001877.pub4.PMID 21249649.
- ^ a b Gulati, AP; Domchek, SM (2008 Jan). "The clinical management of BRCA1 and BRCA2 mutation carriers". Current oncology reports 10 (1): 47–53. doi:10.1007/s11912-008-0008-9. PMID 18366960.
- ^ a b Holland Chp. 40
- ^ Holland Chp.41
- ^ Cassileth BR, Deng G (2004). "Complementary and alternative therapies for cancer". Oncologist 9 (1): 80–9.doi:10.1634/theoncologist.9-1-80. PMID 14755017.
- ^ What Is CAM?National Center for Complementary and Alternative Medicine. retrieved 3 February 2008.
- ^ Vickers A (2004). "Alternative cancer cures: 'unproven' or 'disproven'?". CA Cancer J Clin 54 (2): 110–8.doi:10.3322/canjclin.54.2.110. PMID 15061600.
- ^ "NCCN Guidelines".
- ^ "Clinical Practice Guidelines for Quality Palliative Care". The National Consensus Project for Quality Palliative Care (NCP).
- ^ Levy, MH; Back, A, Bazargan, S, Benedetti, C, Billings, JA, Block, S, Bruera, E, Carducci, MA, Dy, S, Eberle, C, Foley, KM, Harris, JD, Knight, SJ, Milch, R, Rhiner, M, Slatkin, NE, Spiegel, D, Sutton, L, Urba, S, Von Roenn, JH, Weinstein, SM, National Comprehensive Cancer Network (September 2006). "Palliative care. Clinical practice guidelines in oncology". Journal of the National Comprehensive Cancer Network: JNCCN 4 (8): 776–818.PMID 16948956.
- ^ a b Rheingold, Susan; Neugut, Alfred; Meadows, Anna (2003)."156: Secondary Cancers: Incidence, Risk Factors, and Management". In Frei, Emil; Kufe, Donald W.; Holland, James F..Holland-Frei Cancer Medicine (6th ed.). Hamilton, Ont: BC Decker. p. 2399. ISBN 1-55009-213-8. Retrieved 5 November 2009.
- ^ Montazeri A (2009-12-23). "Quality of life data as prognostic indicators of survival in cancer patients: an overview of the literature from 1982 to 2008". Health Qual Life Outcomes 7: 102.doi:10.1186/1477-7525-7-102. PMC 2805623.PMID 20030832.
- ^ "Cancer Facts and Figures 2012". Journalist's Resource.org.
- ^ "WHO Disease and injury country estimates". World Health Organization. 2009. Retrieved Nov. 11, 2009.
- ^ WHO (Oct 2010). "Cancer". World Health Organization. Retrieved 2011-01-05.
- ^ a b Coleman, William B. and Rubinas, Tara C. (2009). "4". In Tsongalis, Gregory J. and Coleman, William L.. Molecular Pathology: The Molecular Basis of Human Disease. Amsterdam: Elsevier Academic Press. p. 66. ISBN 0-12-374419-9.
- ^ Johnson, George (28 December 2010). "Unearthing Prehistoric Tumors, and Debate". The New York Times.
- ^ Pawelec, G; Derhovanessian, E, Larbi, A (2010 Aug). "Immunosenescence and cancer". Critical reviews in oncology/hematology 75 (2): 165–72.doi:10.1016/j.critrevonc.2010.06.012. PMID 20656212.
- ^ Anisimov, VN; Sikora, E, Pawelec, G (2009 Aug). "Relationships between cancer and aging: a multilevel approach". Biogerontology10 (4): 323–38. doi:10.1007/s10522-008-9209-8.PMID 19156531.
- ^ Fraumeni, Joseph F.; Schottenfeld, David; Marshall, James M. (2006). Cancer epidemiology and prevention. Oxford [Oxfordshire]: Oxford University Press. p. 977. ISBN 0-19-514961-0.
- ^ Bostwick, David G.; Eble, John N. (2007). Urological Surgical Pathology. St. Louis: Mosby. p. 468. ISBN 0-323-01970-6.
- ^ a b Kaatsch, P (2010 Jun). "Epidemiology of childhood cancer".Cancer treatment reviews 36 (4): 277–85.doi:10.1016/j.ctrv.2010.02.003. PMID 20231056.
- ^ Ward, EM; Thun, MJ, Hannan, LM, Jemal, A (2006 Sep). "Interpreting cancer trends". Annals of the New York Academy of Sciences 1076: 29–53. Bibcode 2006NYASA1076...29W.doi:10.1196/annals.1371.048. PMID 17119192.
- ^ a b c d e f Hajdu, SI (2011-03-01). "A note from history: landmarks in history of cancer, part 1.". Cancer 117 (5): 1097–102.PMID 20960499.
- ^ Moss, Ralph W. (2004). "Galen on Cancer". CancerDecisions.Moss in turn attributes this reason for the name to Paul of Aegina, 7th Century AD, quoted in Michael Shimkin, Contrary to Nature, Washington, D.C.: Superintendent of Document, DHEW Publication No. (NIH) 79-720, p. 35.
- ^ a b Hajdu, SI (2011-06-15). "A note from history: landmarks in history of cancer, part 2.". Cancer 117 (12): 2811–20.PMID 21656759.
- ^ Yalom, Marilyn (1998). A history of the breast (1st Ballantine Books ed. ed.). New York: Ballantine Books. ISBN 0-679-43459-3.
- ^ Hajdu, SI (2011-07-12). "A note from history: Landmarks in history of cancer, part 3.". Cancer. PMID 21751192.
- ^ Grange JM, Stanford JL, Stanford CA (2002). "Campbell De Morgan's 'Observations on cancer', and their relevance today".Journal of the Royal Society of Medicine 95 (6): 296–9.doi:10.1258/jrsm.95.6.296. PMC 1279913. PMID 12042378.
- ^ Ehrenreich, Barbara (November 2001). "Welcome to Cancerland". Harper's Magazine. ISSN 0017-789X.
- ^ Rapini, Ronald P.; Bolognia, Jean L.; Jorizzo, Joseph L. (2007).Dermatology: 2-Volume Set. St. Louis: Mosby. ISBN 1-4160-2999-0.
- ^ "Skin cancers". World Health Organization. Retrieved 19 January 2011.
- ^ McCulley, Michelle; Greenwell, Pamela (2007). Molecular therapeutics: 21st-century medicine. London: J. Wiley. p. 207.ISBN 0-470-01916-6.
- ^ Gwyn, Richard (1999). "10". In Cameron, Lynne; Low, Graham.Researching and applying metaphor. Cambridge, UK: Cambridge University Press. ISBN 0-521-64964-1.
- ^ Sulik, Gayle (2010). Pink Ribbon Blues: How Breast Cancer Culture Undermines Women's Health. New York: Oxford University Press. pp. 78–89. ISBN 0-19-974045-3. OCLC 535493589.
- ^ a b c Olson, James Stuart (2002). Bathsheba's Breast: Women, Cancer and History. Baltimore: The Johns Hopkins University Press. pp. 145–170. ISBN 0-8018-6936-6. OCLC 186453370.
- ^ a b c d Ehrenreich, Barbara (2009). Bright-sided: How the Relentless Promotion of Positive Thinking Has Undermined America. New York: Metropolitan Books. pp. 15–44. ISBN 0-8050-8749-4.
- ^ "What Is Cancer?". National Cancer Institute. Retrieved 2009-08-17.
- ^ "Cancer Fact Sheet". Agency for Toxic Substances & Disease Registry. 2002-08-30. Retrieved 2009-08-17.
- ^ Wanjek, Christopher (2006-09-16). "Exciting New Cancer Treatments Emerge Amid Persistent Myths". Retrieved 2009-08-17.
- ^ Hayden, Erika C. (2009-04-08). "Cutting off cancer's supply lines". Nature 458 (7239): 686–687. doi:10.1038/458686b.PMID 19360048.
- ^ Sleigh SH, Barton CL (2010). "Repurposing Strategies for Therapeutics". Pharm Med 24 (3): 151–159.doi:10.2165/11536770-000000000-00000.
- ^ Winther H, Jorgensen JT (2010). "Drug-Diagnostic Co-Development in Cancer". Pharm Med 24 (6): 363–375.doi:10.2165/11586320-000000000-00000.
- ^ Sharon Begley (2008-09-16). "Rethinking the War on Cancer".Newsweek. Retrieved 2008-09-08.
- ^ Kolata, Gina (April 23, 2009). "Advances Elusive in the Drive to Cure Cancer". The New York Times. Retrieved 2009-05-05.
- ^ a b c d e f g h i j Connie Henke Yarbro, Debra Wujcik, Barbara Holmes Gobel, ed. (2011). Cancer nursing: principles and practice(7 ed.). Jones & Bartlett Publishers. pp. 901–905. ISBN 978-1-4496-1829-2.
- Holland, James F. (2009). Holland-Frei cancer medicine. (8th ed. ed.). New York: McGraw-Hill Medical. ISBN 978-1-60795-014-1.
Further reading
- Kleinsmith, Lewis J. (2006). Principles of cancer biology. Pearson Benjamin Cummings. ISBN 978-0-8053-4003-7.
- Mukherjee, Siddhartha (16 November 2010). The Emperor of All Maladies: A Biography of Cancer. Simon and Schuster. ISBN 978-1-4391-0795-9.
- Pazdur, Richard; et al. (May 2009). Cancer Management: A Multidisciplinary Approach. Cmp United Business Media. ISBN 978-1-891483-62-2. (online at cancernetwork.com)
- Tannock, Ian (2005). The basic science of oncology. McGraw-Hill Professional. ISBN 978-0-07-138774-3.
- Manfred Schwab (2008). Encyclopedia of Cancer (4 Volume Set). Berlin: Springer. ISBN 3-540-36847-7.
External links
| * | Wikimedia Commons has media related to: Cancer |
- Cancer at the Open Directory ProjectConditionsMalignant progression
- Dysplasia
- Carcinoma in situ
- Cancer
- Metastasis
TopographyHistologyOtherMisc.Carcinogen—Cancer causing materials and agents
No comments:
Post a Comment